Can The Doctor-Patient Relationship Survive?

It’s not enough to understand the issues in this article ? it is important to review them and see what can be changed in the practice to minimize them and ? in some cases ? even make lemonade out of lemons. We find that a 10,000 foot analysis of issues followed by a ground level analysis, often allows for the mitigation or elimination of headaches and costly practice issues.
“I don’t want to be spending my time on the phone getting prior authorizations. I want to be talking to my patients and taking care of them.”
That sentiment, from family physician Reid Blackwelder, MD, FAAFP, president of the American Academy of Family Physicians, captures the feelings of many primary care physicians (PCPs) as they struggle to establish the long-term relationships needed to help patients stay healthy throughout their lives.
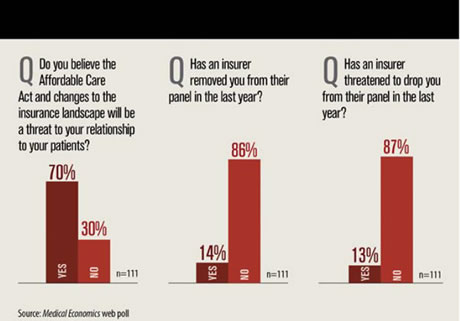
Compounding the sense of frustration is uncertainty over the effects of the Affordable Care Act. Will it bring millions of new patients into the healthcare system, and if so, how will primary care practices accommodate them? Will insurance companies remove PCPs from their panels, forcing patients to change doctors? These are just a few of the unknowns surrounding the far-reaching legislation.
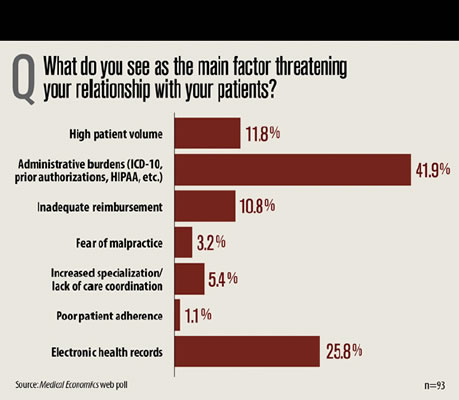
In November, Medical Economics asked readers of its eConsult newsletter to identify what they see as the main threats to their relationships with patients. The number one issue cited was the growing administrative demands from requirements such as converting to the International Classification ofDiseases-10th revision and obtaining prior authorizations from insurance providers for prescriptionsand procedures. That was followed by the use of electronic health records (EHRs), high patientvolume, and inadequate reimbursement.
Assigning routine functions to others
Most such tasks don’t individually require a great deal of time, but together they can add up to a substantial part of a PCP’s workday.
Blackwelder cites a study in the November, 2013 issue of Health Affairs showing that many PCPs could save up to 30 minutes per day assigning other staff members to perform routine functions.
That time could be used to see more patients or spend more time with them. “Either way, it’s improved quality time doing what I’m trained to do, which is care for patients,” he says.Robert Eidus, MD, MBA, a family physician in Cranford, New Jersey, feels his administrative burden has been at a “continuously high” level going back 15 years, although Medicare has added some hurdles in recent years. “It takes time away from what we [providers] do, or we have to hire additional staff, which means we have to see more patients to pay for the staff, which shortens patient visits,” he says.
The issue of time—or the lack of it—underlies many of the concerns cited by both physicians and patients. “The biggest issue I’ve always seen is the lack of time,” says Yul Ejnes, MD, FACP, an internist in Cranston, Rhode Island. “I think doctors and patients have better relationships when they can sit and talk about whatever they need to.”
Eidus calls the situation in which many PCPs find themselves “a hamster wheel, where we’re forced to see more and more patients just to stay afloat financially.” He blames the fee-for-service payment method, under which doctors can only get paid for patient office visits. “There are a lot of things we could do to care for our patients without having them come into the office, except we would go bankrupt,” he says.
“With someone who is a little older and comes to an appointment with four or five issues they want to address, it’s the devil to get through that in 15 or 20 minutes,” says Molly Cooke, MD, FACP, an internist in San Francisco, California and president of the American College of Physicians.Moreover, she says, the physician may have his or her own list of preventive issues to tackle.“Explaining the options for colorectal cancer screening is at least a 5-minute discussion, and if I have six of those [types of topics] that’s the whole visit, and it doesn’t leave time for her to talk about how proud she is of her granddaughter who just graduated from college, all the things that really establish a relationship,” she says. “If I get through my list but we haven’t dealt with what the patient really wanted to talk about, that patient is going to leave unhappy.”
The potential for patient unhappiness is reflected in a 2012 Institute of Medicine discussion paper,“Communicating with Patients on Health Care Evidence.” Asked to complete the statement, “I want my doctor to….” 80% of respondent supplied the words “listen to me.”
Insurers requirements can lead to friction
Tracking the requirements and limitations of insurance providers creates its own class of administrative headaches, and can sometimes lead to friction with patients.
“My patients today have hundreds of permutations of different insurance policies covering different things,” Eidus says. “Sometimes patients discover a service isn’t covered, and now we’re caught between the patient and the insurance company, when all we’re trying to do is provide the best care.”
Worse, sometimes patients ask him to contact the patient’s insurance company to get coverage or a service that may not be medically appropriate, or to change a diagnostic code so that a service will be covered. “We would like to be the patient’s advocate, but we can’t commit insurance fraud,” says. “We don’t like to get between the patient and their insurance company, but sometimes we find we get pulled into disputes anyway.”
A second, frequently-cited doctor-patient barrier stems from EHRs. In some cases the barrier is literal. Many patients complain their doctors focus more attention on the EHR than on the patient. “It can be a major problem when patients feel like they’re the third person in the room, and it’s the doctor and the EHR who are doing most of the interacting,” says Ejnes.
“I’ve had patients who have left their previous doctor because they said that in a 15-minute appointment the doctor spent 10 minutes typing,” says William Blazey, DO, a family practitioner in Old Westbury and Central Islip, New York.
For Blazey, the challenge posed by EHRs stems more from their time demands. He estimates he spends 8 to 10 minutes per chart entering information not directly related to patient care, mainly tied to quality metrics.
“You have to wonder how much quality care you could have given your patients if you weren’t spending that time marking off quality indicators,” he says.
‘Most of the documentation we do is…for billing purposes’
“Most of the documentation we do is not for patient outcomes, but for billing purposes,” saysBlackwelder. “If I’m documenting things to make sure I have all the right checks to support billing, that takes away from my ability to take care of my patients. So if we can find ways of minimizing documentation requirements that don’t affect patient care, it would help us refocus on patients.”Keeping track of and coordinating the care their patients receive from other providers in an increasingly fragmented healthcare system is yet another barrier to patient relationships for PCPs, and it’s frequently made worse by EHRs.
“My system doesn’t talk to Dr. Smith’s system, which doesn’t talk to Dr. Jones’s system, which doesn’t talk to the hospital,” says Jeanne Hungerpiller, MD, a solo general practitioner in Savannah, Georgia who responded to the Medical Economics survey.
Virtually all of Hungerpiller’s communications with specialists and other providers takes place via electronic fax, and requires a staff member to track and follow up on sent and received requests.
“Unfortunately, this breaks down a lot. The other office says they sent the note, but we never received it, and we have to ask for it again. It gets very frustrating,” she says.
“As a primary care doc, one of the cornerstones of what I try to do with my patients is coordinate their care among specialists, especially if it’s a cancer diagnosis or something else that requires multiple specialists,” says Blazey. “Often I find that patients will see a specialist and then forget who they saw so they can’t relay back to me the testing they had done.”
The problem gets compounded, Blazey adds, when a specialist refers a patient to another specialist without informing him. “I might send a doctor to a cardiologist, and by the time the patients comes back to me they’ve also seen a urologist and gastroenterologist. If the patient had had a discussion with me maybe they could have avoided unneeded testing or treatments.”
Patients are better informed
The vast quantity of health and medical-related information available to patients through websites, general-interest media, and direct-to-consumer advertising can also be a source of tension between patients and their doctors.
“My hope is that patients will come in with questions, having done some reading,” says the AAFP’s
Blackwelder. “It makes my role easier in caring for that patient, but it does sometimes require a different mindset for us physicians, because medicine has for a long time been very patriarchal.”
“It cuts both ways,” says Blazey. “Patients do now come in with more information about their medical issues, and knowing some of the lingo helps them navigate the system better. On the other hand, they may have heard on the news someone getting treated for a disorder, but that treatment may not be right for them, and I have to take the time to explain why.“
Like many other issues in doctor-patient relationships, Blazey adds, it comes down to trust, and knowing the patient well.
“When you have that longitudinal relationship with the person, you start to understand them and know the best way to reach them,” he says.
Source: Medicial Economic


















